



Clinical Documentation Made Simple (Volume I)
Clinical Documentation Made Simple (Volume I)
Real SOAP notes, real cases - annotated by a counselor who's written hundreds of them.
Stop letting administrative paperwork drain your clinical energy.
For many mental health practitioners and counselors, "documentation paralysis" is a daily reality. Spending hours staring at a blank screen, worrying about insurance audit rejections, or struggling to articulate your clinical logic can turn a fulfilling practice into an overwhelming chore.
Clinical Documentation Made Simple (Volume I) is a tactical, desk-ready manual engineered to turn defensive note-writing into structured, defensible clinical logic. This guide completely strips away dry academic fluff and replaces it with real-world scaffolding, comparative side-by-side matrices, and micro-level annotations that show you exactly what to write and why it works.
📥 What’s Inside the Guide?
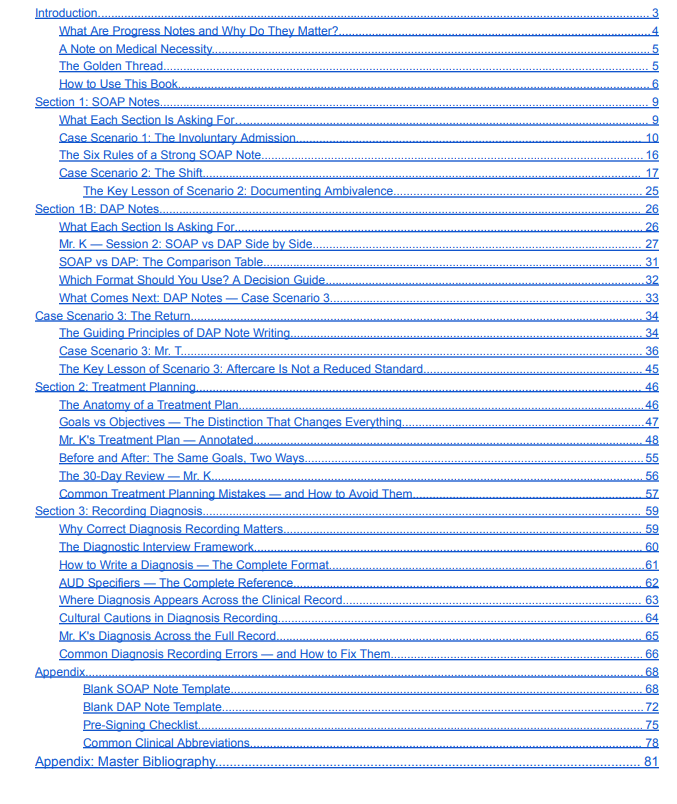
- The "Golden Thread" Framework: Learn how to build an unbroken clinical narrative from intake assessment to discharge summary, seamlessly satisfying state and insurance audit requirements.
- Decoding Medical Necessity: Master the exact language needed to prove functional impairment and justify clinical hours to major managed care organizations.
- SOAP Notes Deep-Dive: Walk through involuntary admission scenarios, step-by-step behavioral tracks, and formal clinical modules (including SCID-5 tracking for Severe Alcohol Use Disorder).
- DAP Notes Mastery: Learn how to isolate subjective reports from objective data and manage nuanced outpatient aftercare dilemmas—featuring structured tracking templates like the SIGECAPS matrix.
- The 24-48 Hour Audit Guard: Operational strategies to streamline your workflow so your notes are legally defensible and completed on time without eating into your personal life.
🛠️ Built for Scannability & Direct Utility
This is not a textbook; it is an operational toolkit. It features:
- Side-by-Side Comparison Tables that sharply separate clinical observations from client statements.
- Annotated Case Tracks (following longitudinal patient progress across multiple sessions) to help you visualize client trajectory.
- Person-First Language Safeguards to ensure your charting stays entirely non-stigmatizing and ethically compliant.
👥 Who Is This Manual For?
- Early-Career Counselors & Resident Counselors.
- Addiction Treatment & Substance Use Specialists.
- Social Workers & Private Practice Therapists.
- Psychiatric Nurses.
Stop writing notes at midnight. Before your next session starts, let's get this right.
👉 Click "Buy Now" to download your copy instantly and upgrade your clinical charting today!