

If you have ADHD, the chance that you also have dyslexia, autism, or DCD (developmental coordination disorder) is far higher than chance. If you’re autistic, the same is true for ADHD, epilepsy, and hypermobility. These aren’t random coincidences—they reflect a core fact about human brains: neurotypes overlap because biology overlaps.
Yet most diagnostic systems, school supports, and even workplace accommodations treat each condition as if it exists in a silo. That mismatch between biological reality and institutional structure causes real harm: missed diagnoses, conflicting advice, and people feeling like they’re “too complex” to fit neatly into any box.
In this post, I’ll walk through:
- What neurodiversity means (and doesn’t mean), updated with current neuroscience.
- Why co-occurrence is the rule, not the exception.
- A revised set of neurodiversity definitions that respect both the neurodiversity paradigm and the biology.
- How the APA’s Inclusive Language Guide (2023) now supports neurodiversity-affirming language.
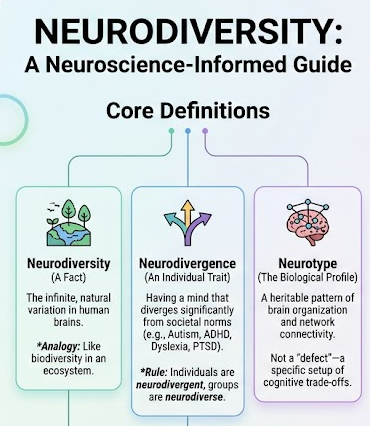
Neurodiversity Is a Biological Fact – Not a Belief or a Movement
One of the most persistent confusions is using “neurodiversity” to mean the neurodiversity paradigm or the Neurodiversity Movement. As Nick Walker (2021) has carefully explained, neurodiversity is simply the infinite variation in human neurocognitive functioning—just as biodiversity is the variation in life forms.
Neuroscience update:
Neurodiversity arises from genome-driven differences in:
- Synaptic pruning and dendritic arborization.
- Neurotransmitter tone (dopamine, GABA, glutamate, norepinephrine).
- Large-scale brain network connectivity (default mode, salience, central executive, sensorimotor).
- Temporal processing and neural noise.
No two human brains are identical, and the range of “typical” functioning is much narrower than the range of human neurobiology (Astle et al., 2022).
✅ Correct usage: “Our school’s curriculum is designed to accommodate neurodiversity.”
❌ Incorrect usage: “My neurodiversity makes it hard to focus.” (That’s neurodivergence.)
Neurotypical (NT)
Definition (updated with allistic distinction):
Having a style of neurocognitive functioning that falls within the dominant societal standards of “normal” – meaning no diagnosis or recognized neurotype that significantly diverges from population norms on attention, language, motor, social, or sensory dimensions. Neurotypical people are one subset of allistic people (non‑autistic), but not all allistic people are neurotypical.
Neuroscience update:
Neurotypicality is not a “baseline” brain – it is one region on the neurodiversity spectrum, with its own genetic architecture and trade‑offs (e.g., lower risk for certain learning differences but potentially less cognitive flexibility in specific domains).
Correct usage:
- ✅ “She is neurotypical – she does not have any neurodivergent condition.”
- ✅ “He is allistic but not neurotypical; he has ADHD.”
- ❌ “Is your daughter autistic or neurotypical?” (Incorrect – she could be allistic but not neurotypical, e.g., dyslexic.)
Allistic
Definition (community + neuroscience):
A person who is not autistic. The term includes both neurotypical people and non‑autistic neurodivergent people (e.g., a person with ADHD or dyslexia who is not autistic). Allistic is not a synonym for neurotypical – it simply means “without autism.”
Origin:
Coined by the autistic community in the early 2000s to avoid the imprecise and sometimes oppositional framing of “non‑autistic.” The term is widely used in autistic self‑advocacy spaces, including the Neurodiversity Movement (Walker, 2021).
Neuroscience note:
From a neurobiological perspective, “allistic” is a negative category – it defines what someone is not (autistic), not a specific brain type. Allistic brains do not share a single neural profile; they range from neurotypical to other neurotypes (ADHD, dyslexia, etc.). Therefore, allistic is a useful social‑identity term but not a neurotype itself.
Correct usage examples:
- ✅ “Both autistic and allistic students benefit from clear written instructions.”
- ✅ “She is allistic but has ADHD and dyscalculia.”
- ❌ “He is allistic, so he must be neurotypical.” (Incorrect – allistic includes many neurodivergent people.)
Why this term matters: Before “allistic,” writers often used “non‑autistic” (which centers autism as the reference point) or incorrectly used “neurotypical” to mean “not autistic.” This erased neurodivergent allistic people – for example, a dyslexic person who is not autistic is allistic but not neurotypical. Using “allistic” precisely respects both autism and other neurotypes.
Neurodivergent / Neurodivergence – An Individual Trait, Not a Euphemism for Autism
Coined by Kassiane Asasumasu in 2000, neurodivergent means having a mind that functions in ways that diverge significantly from dominant societal norms of “normal.” This includes both innate neurotypes (autism, dyslexia, ADHD) and acquired neurodivergence (TBI, PTSD, some forms of epilepsy).
Neurodivergent (adj.) / Neurodivergence (n.)
From the NNLM (2026): “People who identify themselves as neurodivergent typically have one or more conditions… but there are no medical criteria or definitions of what it means to be neurodivergent.”
Neuroscience definition:
A state of neurocognitive functioning that diverges significantly from population norms on one or more dimensions (attention, language, motor, social, sensory, emotion regulation), arising from genetic, epigenetic, and/or experience‑dependent neuroplasticity. Neurodivergence is typically lifelong, though its expression changes across development and contexts. It is not a disorder of a “normal” brain but rather a natural, heritable variation in human brain organization. Co‑occurrence of multiple neurotypes is expected, not exceptional.
Key NNLM principle: Differences are not deficits. There is no one “right” way of thinking, learning, or behaving.
Neurodivergence is typically:
- Highly heritable (e.g., 50–80% for most common neurotypes).
- Stable across the lifespan, though expression changes with development and environment.
- Characterized by trade-offs, not just deficits. For example, dyslexic brains show enhanced peripheral vision, narrative reasoning, and big-picture pattern detection (Schneps et al., 2012).
✅ Correct: “She is neurodivergent; she’s autistic and has ADHD.”
❌ Incorrect: “He is neurodiverse.” (Individuals cannot be “diverse.”)
Neurotype – The Biology-Based Category We’ve Been Missing
A neurotype is a recognizable, heritable pattern of brain organization and information processing. Think of it like a “brain profile” rather than a disorder.
Neuroscience definition (modeled on IDA 2025):
A neurotype is a pattern of neurobiological organization and information processing that arises from complex interactions among genetic, epigenetic, and environmental influences across development. Neurotypes exist along continua of cognitive, sensory, and affective attributes, and they co-occur at rates predicted by shared polygenic liabilities and overlapping brain circuit vulnerabilities.
Examples:
- Dyslexia: Atypical development of left-hemisphere posterior reading networks (temporo-parietal and occipito-temporal), often with compensatory right-hemisphere engagement. Heritability ~50–70%. Co-occurs with ADHD (30–50%) and DCD (30–60%).
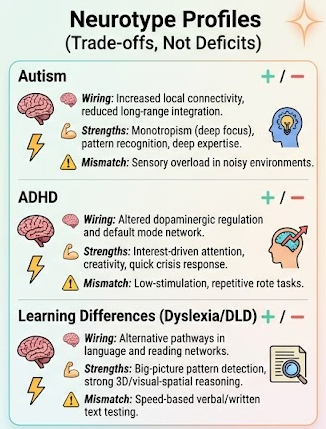
- ADHD: Altered frontostriatal, frontoparietal, and default mode network connectivity; differences in dopamine and norepinephrine regulation. Heritability ~70–80%. Co-occurs with autism (40–70%) and dyslexia (30–50%).
- Autism: Increased local but reduced long-range cortical connectivity, altered excitatory/inhibitory balance (GABA/glutamate), and differences in social reward circuitry. Heritability ~80%. Co-occurs with ADHD (40–70%), epilepsy (5–30%), and hypermobility syndromes.
No single biomarker defines any neurotype. But the pattern of network differences, co-occurrence rates, and heritability is robust across studies.
Autism Spectrum Disorder (ASD) / Autism Spectrum Condition (ASC)
Neurotype definition (autism as a neurotype):
A neurotype involving atypical neural connectivity – typically increased local connectivity with reduced long‑range cortical integration – and altered excitatory/inhibitory (E/I) balance (GABA/glutamate). Differences are prominent in social reward circuitry (striatum, medial prefrontal cortex), sensory processing networks, and attentional orienting systems.
- Heritability: ~80% (polygenic, many rare variants)
- Key features: Monotropism (intense, deep focus), systemizing, sensory hyper‑ or hypo‑responsivity, delayed or atypical social communication (not absence of social interest), strong pattern recognition.
- Co‑occurrence: ADHD (40–70%), epilepsy (5–30%), hypermobility/Ehlers‑Danlos syndromes, gastrointestinal conditions, anxiety.
- Strengths/trade‑offs: High attention to detail, loyalty, deep expertise in areas of interest. Sensory overload and social mismatch in neurotypical‑dominated environments are environmental, not intrinsic, deficits.
Language note: Identity‑first (“autistic person”) is preferred by the majority of autistic adults (APA, 2023). Avoid “person with autism” unless an individual requests it.
Attention Deficit Hyperactivity Disorder (ADHD)
Neurotype definition (ADHD as a neurotype):
A neurotype characterized by differences in dopaminergic and noradrenergic regulation, particularly in frontostriatal, frontoparietal, and default mode networks. These differences affect reward processing, time perception, working memory, and cognitive regulation (executive functions). Importantly, ADHD is not a “deficit of attention” but a variable, interest‑driven attention system – attention is often exceptionally intense for engaging tasks.
- Heritability: ~70–80% (highly polygenic)
- Key features: Interest‑based nervous system, creative nonlinear thinking, resilience under pressure, high energy, emotional intensity (rejection sensitive dysphoria is common but not universal).
- Co‑occurrence: Autism (40–70%), dyslexia (30–50%), DCD (50–60%), anxiety, depression.
- Strengths/trade‑offs: Quick crisis response, idea generation, hyperfocus on passions. Difficulty with rote, low‑stimulation tasks and societal expectations of consistent “on‑demand” attention.
Language note: “ADHDer” or “person with ADHD” are both acceptable. Avoid “suffers from ADHD” (APA, 2023).
Down Syndrome (Trisomy 21)
Neurotype definition (Down syndrome as a neurotype):
A neurotype caused by the presence of all or part of an extra copy of chromosome 21, leading to altered brain development including reduced cortical volume, smaller cerebellum, and atypical hippocampal formation. These neurobiological differences produce a distinctive cognitive profile: relative strengths in visual‑spatial processing, social reasoning, and emotional intelligence, with more variable challenges in verbal working memory and sequential processing.
- Heritability: Not heritable in the usual polygenic sense – it is a chromosomal condition (95% trisomy 21). However, it is a lifelong, innate neurotype.
- Key features: High social motivation, empathy, routine‑based learning, musicality, strong long‑term memory.
- Co‑occurrence: Autism (~20%), ADHD, sleep apnea, early‑onset Alzheimer’s pathology (by midlife).
- Strengths/trade‑offs: Remarkable social warmth and perseverance. Increased risk for specific health conditions, but neurodiversity framework rejects framing the person as a “tragedy” or solely by medical complications.
Language note: Most adults with Down syndrome prefer identity‑first (“Down syndrome person” or “person with Down syndrome” – always ask). Avoid “Down’s child” (possessive) or “suffers from Down syndrome.” The NNLM includes Down syndrome as a neurotype in its list, consistent with the view that intellectual disability is not a defect but a difference.
Learning Differences (Specific Learning Disorders, e.g., Dyslexia, Dyscalculia, Dysgraphia)
Neurotype definition (learning differences as a neurotype family):
A group of neurotypes involving atypical development of brain networks specialized for academic skills (reading, writing, mathematics), despite typical or above‑typical intelligence in other domains. These are not “delays” but alternative neural pathways. For example, dyslexic brains show reduced left‑hemisphere temporo‑parietal and occipito‑temporal activation during reading, with compensatory right‑hemisphere and frontal engagement. Dyscalculia involves altered parietal intrasulcal connectivity for number sense.
- Heritability: 50–80% depending on the specific learning difference.
- Key features: Dyslexia – enhanced peripheral vision, big‑picture pattern detection, narrative reasoning. Dyscalculia – strong spatial reasoning, creativity, verbal skills. Dysgraphia – oral creativity, problem‑solving.
- Co‑occurrence: ADHD (30–50% for dyslexia), DCD, language disorders.
- Strengths/trade‑offs: Learning differences confer trade‑offs (e.g., dyslexic entrepreneurs overrepresented in design, engineering, and storytelling). Difficulties are context‑dependent: text‑heavy, timed environments create mismatch; multisensory, strength‑based environments allow flourishing.
Language note: Use “specific learning difference” or “learning difference” rather than “learning disability” if the individual prefers (UK English often uses “disability”; US neurodiversity advocates often use “difference”). Avoid “learning disabled” as a global label.
Dyslexia
Neurotype definition (dyslexia as a neurotype):
A neurotype involving atypical development of left‑hemisphere posterior reading networks, particularly the temporo‑parietal (phonological assembly) and occipito‑temporal (word form) regions. These differences are present before reading instruction and persist across the lifespan. Dyslexic brains show reduced activation in these areas during reading tasks, with compensatory engagement of right‑hemisphere and frontal regions. This is not a “wiring defect” but an alternative neural architecture that trades efficient automatic word recognition for enhanced peripheral vision, big‑picture pattern detection, and narrative reasoning.
- Heritability: ~50–70% (polygenic; candidate genes affect neuronal migration and axon guidance – e.g., DCDC2, KIAA0319, ROBO1)
- Key neural features:
- Reduced gray matter volume in left occipito‑temporal cortex (“visual word form area”)
- Atypical white matter connectivity in left arcuate fasciculus and inferior longitudinal fasciculus
- Altered rapid auditory and visual processing timing (millisecond‑range differences)
- Preserved or enhanced right‑hemisphere visuospatial networks
- Cognitive profile (trade‑offs, not just deficits):
- Challenges: Slow, effortful word decoding; spelling inconsistency; difficulty with rapid naming of symbols (letters, numbers); reduced automaticity in reading fluency.
- Strengths (well‑replicated): Enhanced peripheral vision (Schneps et al., 2012); superior big‑picture/boundary‑detection in visual scenes; strong narrative reasoning and storytelling; high entrepreneurial and design thinking rates (overrepresented in architecture, engineering, and creative fields).
- Co‑occurrence: ADHD (30–50%), DCD (30–60%), dyscalculia (20–40%), specific language impairment.
- Lifespan course: Reading difficulties persist but can be compensated; strengths often become more visible in adulthood when environment allows strength‑based roles.
- Language note: Most dyslexic adults prefer “dyslexic” (identity‑first) over “person with dyslexia.” Avoid “dyslexic sufferer” or “afflicted with dyslexia.” The term “specific learning difference” is often preferred over “disability” in UK and neurodiversity contexts, but “disability” is legally accurate in the US for accommodation rights – let the individual choose.
Key clinical vs. neurodiversity distinction:
DSM‑5 frames dyslexia as a “disorder” based on academic underachievement. The neurotype model reframes it as a brain organization that is poorly matched to print‑heavy, speed‑based instruction – a mismatch, not an intrinsic deficit.
Dysgraphia
Neurotype definition (dysgraphia as a neurotype):
A neurotype involving differences in the neural systems that support handwriting, letter formation, and written expression, typically including the left premotor cortex, supplementary motor area, and the cerebellum – regions involved in motor planning, sequential movement, and orthographic loop feedback (visual‑to‑motor integration). Dysgraphia is not a fine‑motor general deficit; many people with dysgraphia can draw, type, or perform skilled manual tasks normally. The bottleneck is translating language into written symbols automatically – often accompanied by preserved oral storytelling and verbal creativity.
- Heritability: Less studied; estimated 30–50% with significant polygenic overlap with dyslexia and DCD.
- Key neural features:
- Reduced activation in left premotor and superior parietal regions during writing tasks
- Atypical cerebellar and basal ganglia involvement in sequential motor learning
- Differences in the “orthographic loop” (visual feedback to motor output)
- Typically intact language generation (speaking) networks
- Cognitive profile (trade‑offs, not just deficits):
- Challenges: Illegible or inconsistent handwriting; extreme effort/pain when writing by hand; trouble with spacing, sizing, and staying on line; often slow or unintelligible handwriting even when copying; written composition far below oral composition ability.
- Strengths (well‑reported, under‑researched): High verbal creativity; strong oral storytelling; ability to produce complex ideas when using speech‑to‑text or typing; often skilled in visual arts, design, or other fine‑motor activities that do not require sequential letter formation.
- Co‑occurrence: Dyslexia (30–60%), DCD (50–70%), ADHD (30–50%), specific language impairment.
- Lifespan course: Handwriting remains effortful for most adults, but typing and speech recognition circumvent the bottleneck. Many adults with dysgraphia report that school handwriting trauma affected self‑esteem, while oral or typed expression reveals their true ability.
- Language note: “Dysgraphic” as an identity term is uncommon; most prefer “person with dysgraphia.” Be aware that dysgraphia is often confused with “developmental coordination disorder (DCD)” – they co‑occur but are distinct (DCD affects gross and fine motor planning broadly; dysgraphia is specific to written symbol production).
Key clinical vs. neurodiversity distinction:
In schools, dysgraphia is often treated as a “handwriting disorder.” The neurotype model recognizes it as a specific bottleneck in the written output channel – not a reflection of intelligence, effort, or general motor ability.
Dyscalculia
Neurotype definition (dyscalculia as a neurotype):
A neurotype involving atypical development of the intraparietal sulcus (IPS) – the brain region specialized for quantity processing, number sense, and magnitude comparison. Dyscalculic brains show reduced IPS gray matter volume, reduced functional activation during numerical tasks, and altered connectivity between IPS and prefrontal working memory regions. This is not a generalized math “weakness” but a specific difference in the preverbal “number sense” that underlies arithmetic. Critically, many people with dyscalculia have preserved or superior reasoning, logic, and verbal skills – they can learn higher mathematics through verbal and spatial strategies, but not through automatic quantity intuition.
- Heritability: ~50–60% (polygenic; candidate genes include some overlap with dyslexia – e.g., ROBO1 – but distinct genetic architecture)
- Key neural features:
- Reduced gray matter volume and resting-state connectivity in bilateral IPS (especially left)
- Atypical functional activation in IPS during quantity comparison (e.g., judging which of two numbers is larger)
- Altered connectivity between IPS and dorsolateral prefrontal cortex (working memory)
- Intact or enhanced verbal and visual‑spatial networks for non‑numerical information
- Cognitive profile (trade‑offs, not just deficits):
- Challenges: Poor quantity estimation (e.g., approximate number system – judging which group has more items without counting); difficulty with arithmetic fact retrieval (e.g., multiplication tables); trouble with subitizing (instantly seeing how many items are in a small set); number reversals or misordering; difficulty with time estimation, financial planning, and direction‑following that involves magnitude (e.g., “which is closer?”).
- Strengths (emerging evidence, clinically significant): Strong verbal reasoning and narrative thinking; creative problem‑solving in non‑numerical domains; often excellent at geometry (spatial but non‑quantitative) and qualitative logic; higher‑than‑expected representation in arts, law, writing, and narrative‑driven professions. Many adults with dyscalculia report that once numbers are removed, they solve complex logical problems as well as or better than peers.
- Co‑occurrence: Dyslexia (20–40%), ADHD (30–50%), developmental language disorder (20–30%), dyspraxia/DCD (20–30%).
- Lifespan course: Core number‑sense differences persist, but many adults develop compensatory verbal, calculator‑based, or spreadsheet strategies. Difficulties with tasks like splitting a check quickly, estimating grocery costs, or reading analog clocks may remain – these are environmental mismatches, not intellectual failures.
- Language note: “Dyscalculic” as an identity‑first term is emerging but less common than “person with dyscalculia.” Avoid “math dyslexia” (dyscalculia and dyslexia are neurobiologically distinct, though they co‑occur). Because dyscalculia is less well known than dyslexia, a brief explanation is often needed in advocacy settings.
Key clinical vs. neurodiversity distinction:
Schools often treat math difficulty as general “low ability.” The neurotype model shows a domain‑specific difference – people with dyscalculia can excel in complex reasoning, logic, and verbal fields as long as numerical quantity is not the bottleneck.
Dyspraxia / Developmental Coordination Disorder (DCD)
Neurotype definition (DCD/dyspraxia as a neurotype):
A neurotype involving atypical development of cerebellar, basal ganglia, and sensorimotor cortical networks – the brain systems responsible for motor planning, sequencing, timing, and procedural learning. Dyspraxic brains show reduced cerebellar volume, altered connectivity between cerebellum and premotor cortex, and differences in the automaticity of learned motor sequences. This is not clumsiness or laziness; it is a specific difficulty in automating motor routines, which affects everything from handwriting and tying shoes to riding a bike and navigating crowded spaces. Importantly, gross motor skills (running, jumping) and fine motor skills (drawing, buttoning) are both affected, but the cognitive load of performing these actions remains high even after repeated practice.
- Heritability: ~50–70% (polygenic; candidate genes involved in neurite outgrowth and synaptic plasticity)
- Key neural features:
- Reduced cerebellar gray and white matter volume (particularly Crus I/II and lobules involved in motor sequence learning)
- Atypical activation in basal ganglia (putamen) and supplementary motor area during motor imagery and execution
- Reduced functional connectivity between cerebellum and dorsolateral prefrontal cortex – meaning cognitive resources must be consciously allocated to movements that others perform automatically
- Intact or enhanced verbal and higher‑order planning networks (executive function)
- Cognitive profile (trade‑offs, not just deficits):
- Challenges: Difficulty learning new motor skills (e.g., sports, musical instruments, typing); poor handwriting (often co‑occurs with dysgraphia); trouble with balance, catching, or navigating crowds; difficulty with multi‑step physical tasks (e.g., tying laces, using cutlery); slow or inconsistent performance on timed motor tasks; often bumps into objects or people without intention.
- Strengths (well‑reported, under‑researched): High verbal creativity; strong strategic and meta‑cognitive thinking (because they cannot rely on automatic movement, many develop deliberate, plan‑based approaches); empathy and patience from lived experience of being misunderstood; often excellent in fields that require verbal reasoning, design, or long‑term strategy (e.g., law, writing, architecture, research).
- Co‑occurrence: ADHD (50–70%), dyslexia (30–50%), dysgraphia (50–70%), autism (20–30%), developmental language disorder (20–40%).
- Lifespan course: Motor difficulties persist, but many adults develop extensive compensatory strategies (e.g., choosing jobs without fine‑motor demands, using voice typing, avoiding certain physical activities). The hidden cost is high cognitive effort – tasks that are automatic for others remain effortful, leading to exhaustion in environments that require constant fine motor output (e.g., school, office paperwork).
- Language note: “Dyspraxic” is the preferred identity‑first term in the UK and among many self‑advocates. “Person with DCD” is more clinical and preferred in some research contexts. In the US, “DCD” is the diagnostic label, but “dyspraxia” is more common in community and neurodiversity spaces. Avoid “clumsy,” “lazy,” or “uncoordinated” – these are ableist descriptions of a neurobiological reality.
Key clinical vs. neurodiversity distinction:
The DSM‑5 frames DCD as a “disorder” of motor coordination that interferes with daily living. The neurotype model reframes it as a difference in motor automaticity – the person can perform most actions, but only with deliberate, effortful cognitive control rather than unconscious procedural memory. This mismatch becomes disabling in speed‑based, motor‑heavy environments, but not in environments that respect verbal or strategic strengths.
Developmental Language Disorder (DLD)
Neurotype definition (DLD as a neurotype):
A neurotype involving atypical development of left‑hemisphere language networks, particularly the inferior frontal gyrus (Broca’s area, for grammar/syntax) and superior temporal gyrus (Wernicke’s area, for comprehension). DLD is present from birth, persists across the lifespan, and affects the acquisition and use of language in the absence of other explanatory conditions (e.g., hearing loss, intellectual disability, autism). Critically, DLD is not a global cognitive deficit – non‑verbal IQ, visual reasoning, and social motivation are typically within the average range or above. The bottleneck is specifically in phonological working memory, grammatical rule learning, and word retrieval.
- Heritability: ~50–70% (polygenic; candidate genes include FOXP2, CNTNAP2, and ATP2C2 – some overlap with dyslexia and autism)
- Key neural features:
- Reduced gray matter volume in left inferior frontal gyrus (pars triangularis and opercularis) and left superior temporal gyrus
- Atypical white matter connectivity in the left arcuate fasciculus (which connects frontal and temporal language regions)
- Reduced functional activation during grammatical processing and rapid phonological tasks
- Intact non‑verbal processing networks (visual reasoning, pattern recognition)
- Cognitive profile (trade‑offs, not just deficits):
- Challenges (persistent, but modifiable with support): Difficulty understanding complex sentences (e.g., passive voice, embedded clauses); trouble learning verb tenses, prepositions, or grammatical rules implicitly; word‑finding difficulties (“tip of the tongue” often); reduced phonological working memory (difficulty repeating long non‑words or following multi‑step verbal instructions); slower verbal response times.
- Strengths (well‑documented, often overlooked): Strong visual and spatial reasoning; excellent pattern detection in non‑language domains (e.g., puzzles, graphs, visual art); creative problem‑solving; often high social motivation and empathy (unlike some communication profiles in autism – DLD is not a social disorder); many adults with DLD thrive in visual or hands‑on fields (design, engineering, art, trades) and in roles that value written over spoken communication when given time.
- Co‑occurrence: Dyslexia (50–70% – high overlap), ADHD (30–50%), dyspraxia/DCD (20–40%), developmental speech sound disorders (frequent).
- Lifespan course: Language differences persist, but many adults develop powerful compensation – they become excellent written communicators (because writing allows time to retrieve words), skilled listeners, and creative visual thinkers. The “hidden” aspect of DLD (no visible markers) often leads to others assuming they are not trying or are less intelligent – a classic environmental mismatch.
- Language note: “Person with DLD” is the preferred person‑first term (DLD community has expressed strong preference for person‑first, unlike autism). Avoid “language impairment” or “language disorder” without context. Never use “dysphasia” (outdated, confused with aphasia). Because DLD is less known than many other neurotypes, advocacy requires brief explanation: “a specific, lifelong difference in learning and using grammar and vocabulary, with normal intelligence and no hearing or social reasoning problems.”
Key clinical vs. neurodiversity distinction:
The clinical label “Developmental Language Disorder” (replacing “Specific Language Impairment”) is relatively new (CATALISE consensus, 2017). The neurotype model adds that DLD is not a deficit but a specific bottleneck in implicit grammatical learning – the person can learn language explicitly (e.g., rules taught through examples), but not automatically from immersion. This makes early, explicit language support an accommodation, not a cure.
Giftedness (intellectual giftedness as a neurotype)
Neurotype definition:
Giftedness is a neurotype characterized by atypical neurodevelopmental trajectories involving heightened neural efficiency, enhanced connectivity in large‑scale brain networks (particularly prefrontal, parietal, and default mode regions), and distinct patterns of sensory, emotional, and cognitive responsiveness. Gifted individuals show faster neural processing speed, greater working memory capacity, and increased cortical thickness or connectivity in regions supporting abstract reasoning, pattern detection, and complex problem‑solving – but these differences are highly heterogeneous and not reducible to a single biomarker.
- Heritability: ~50–80% (polygenic; overlaps partially with cognitive ability genes but distinct from other neurotypes)
- Key neural features:
- Increased efficiency of prefrontal‑parietal networks (involved in working memory and fluid reasoning)
- Atypical default mode network connectivity (associated with self‑generated thought, creativity, and integrative thinking)
- Faster neural adaptation to novel stimuli (sensory and cognitive)
- Often, but not always, higher global brain volume or cortical thickness in specific regions (not a requirement)
- Cognitive profile (heterogeneous, not monolithic):
- Common traits: Rapid pattern detection, advanced abstract reasoning, large working memory capacity, intense curiosity, early and deep vocabulary (in verbally gifted), strong visual‑spatial reasoning (in spatially gifted), ability to hold multiple complex variables simultaneously.
- Challenges (asynchrony): Uneven development across domains (e.g., advanced cognition with average or delayed social‑emotional or motor skills), sensory overresponsivity, existential concerns at young ages, perfectionism, difficulty with rigid or rote instruction.
- Co‑occurrence with other neurotypes (critical):
- Giftedness co‑occurs with other neurotypes at rates far above chance. Most commonly:
- Autism (significant overlap – “autistic giftedness” is common, not rare)
- ADHD (high overlap; giftedness can mask or interact with attention differences)
- Dyslexia (many gifted individuals are dyslexic – “stealth dyslexia”)
- DCD/dyspraxia (asynchrony includes motor differences)
- Sensory processing differences (hyper‑ or hypo‑sensitivity)
- Strengths/trade‑offs:
- Giftedness is not purely advantageous. Heightened neural sensitivity can lead to overexcitabilities (emotional, intellectual, sensory, psychomotor, imaginational) – intense experiences that are valuable but can be overwhelming without appropriate support. The same neural efficiency that enables rapid learning can also lead to intolerance for slow pacing, boredom, and social mismatch in typical environments.
- Lifespan course:
- Giftedness persists across the lifespan, but its expression is shaped by environment, opportunity, and support. Gifted individuals who lack access to like‑ability peers, challenging curriculum, or understanding of their neurotype often experience underachievement, masking, or mental health difficulties (anxiety, depression). When well‑matched, gifted adults thrive in complex, creative, or research‑intensive fields.
Language note:
Most gifted adults who are aware of their neurotype prefer “gifted person” or “gifted individual” (identity‑first) over “person with giftedness,” though neither is highly politicized. Avoid “gifted and talented” (educational program label) when speaking about neurotype. Crucially – giftedness is not an achievement or a reward. It is a neurobiological pattern of processing information, with both strengths and challenges.
Key neurodiversity framing:
Giftedness is a natural, heritable neurotype – not a “better” way of being, and not a guarantee of success. Under the neurodiversity paradigm, giftedness belongs alongside autism, ADHD, and dyslexia as one form of human neurocognitive variation. It is not superior to other neurotypes, nor is it a “compensation” for a disability. It simply is – with its own profile of trade‑offs.
Twice‑Exceptional (2e) – Outdated Term (Retained for Awareness)
Twice‑Exceptional / 2e (outdated, clinical/historical)
Definition (historical/clinical):
A label that emerged in gifted education to describe a person identified as gifted (high cognitive ability, typically >90th–95th percentile on IQ or achievement) and also having one recognized disability or neurotype (e.g., dyslexia, ADHD, autism, DCD). The “two” refers to two exceptionalities: one above average (gifted) and one below average (disability).
Why this term is now considered outdated (neuroscience and neurodiversity reasons):
- False binary of “two.” Neurobiological reality rarely stops at two. Most people who are both gifted and, say, autistic also have co‑occurring ADHD, anxiety, sensory differences, or other neurotypes. “Twice” artificially limits to two and implies that having more than two is exceptional rather than expected.
- Giftedness is itself a neurotype. Under the neurodiversity framework (and consistent with the definition above), giftedness is a heritable neurobiological pattern – not an “add‑on” to a “normal” brain. Framing giftedness + another neurotype as “2e” implies the other neurotype is a problem layered on top of a gift, rather than two coexisting neurotypes.
- Deficit‑laden framing. The term emerged from special education and gifted education silos, where “exceptional” meant either “gifted” or “disabled.” Combining them as “twice‑exceptional” still centers exceptionality in relation to norms, not neurobiological reality.
- Excludes multiply neurodivergent people. A person who is gifted, autistic, and dyslexic (three neurotypes) does not fit “2e” – yet this profile is common. The term forces a choice of which two to name, erasing the full person.
When you might still see “2e” used:
- In legacy educational systems and IEP documents (US public schools still use 2e as a category).
- In clinical psychology reports (often out of habit, not precision).
- In parenting communities familiar with the term but not yet exposed to “multiply neurodivergent.”
Language guidance:
If you must use “2e” for clarity in a specific context (e.g., school meeting), pair it with an explanation: “This child is twice‑exceptional (2e) – gifted and also has ADHD. More accurately, they are multiply neurodivergent, as giftedness itself is a neurotype and co‑occurrence is expected.” In most writing, prefer multiply neurodivergent (see below).
Multiply Neurodivergent – Preferred, Accurate Term
Multiply Neurodivergent
Definition (neuroscience + community):
A person whose neurocognitive functioning diverges from dominant societal norms in two or more ways – meaning they have two or more neurotypes (e.g., gifted + autistic, or ADHD + dyslexic + gifted). The term explicitly includes giftedness as one of those neurotypes. “Multiply neurodivergent” does not privilege any one neurotype as “primary” or “secondary,” and it does not impose an artificial limit of two.
Neuroscience basis for multiply neurodivergent:
As shown in the co‑occurrence map (Kirby, Do‑IT Solutions, 2024), having multiple neurotypes is the rule, not the exception. Shared genetic variants (pleiotropy) and overlapping brain circuits mean that if you have one neurotype, the probability of having at least one other is significantly elevated. Giftedness shares genetic and neural overlaps with autism, ADHD, and specific learning differences. Therefore, a person who is gifted and autistic is not an unusual “twice‑exceptional” case – they are a typical example of multiply neurodivergent co‑occurrence.
Correct usage examples:
- ✅ “She is multiply neurodivergent: gifted, autistic, and dyspraxic.”
- ✅ “Many students who were previously labeled 2e are more accurately described as multiply neurodivergent, because giftedness is itself a neurotype and co‑occurrence often involves more than two.”
- ❌ “He is 2e – gifted and ADHD.” (Not incorrect in legacy terms, but less accurate and potentially limiting.)
Relationship to giftedness definition (explicit): Because we now define giftedness as a neurotype (see above), a person who is gifted and also has ADHD is simply a multiply neurodivergent person with two neurotypes. If they also have dyslexia, they are multiply neurodivergent with three. No special “2e” category is needed – the same framework that describes autistic+ADHD (two neurotypes) also describes gifted+dyslexic (two neurotypes).
Language note:“Multiply neurodivergent” is preferred by most neurodiversity advocates and is consistent with the APA (2023) guidance to avoid hierarchical or deficit‑centric labels. When speaking about a specific person, always ask if they have a preference – some who grew up with “2e” may still use it for personal identity, but the field is moving toward “multiply neurodivergent.”
Example of Language Shift in Practice
Old (2e, outdated):
“My son is twice‑exceptional (2e). He is gifted and also has autism.”
New (multiply neurodivergent, accurate):
“My son is multiply neurodivergent. He is gifted and autistic – both are neurotypes, not one a gift and the other a deficit. He also has dyspraxia, so three neurotypes overall.”
Prader‑Willi Syndrome (PWS)
Neurotype definition (Prader‑Willi syndrome as a neurotype):
A neurotype caused by the loss of paternally expressed genes on chromosome 15q11.2‑q13.1 (via deletion, uniparental disomy, or imprinting defect). This affects hypothalamic development, leading to a distinctive neuroendocrine and cognitive profile: persistent hunger sensation (hyperphagia) driven by hypothalamic dysregulation, low resting metabolic rate, and a specific cognitive pattern including strengths in jigsaw‑puzzle‑type visual matching, long‑term memory, and verbal reasoning, alongside challenges with abstract math and executive function.
- Heritability: Not heritable in the usual sense – it is an imprinting disorder, but once present, it is a lifelong neurotype.
- Key features: High social motivation, good verbal skills, love of routine and puzzles, emotional sensitivity.
- Co‑occurrence: Autism‑like social traits (~25%), obsessive‑compulsive behaviors, sleep disorders, psychosis risk in young adulthood.
- Strengths/trade‑offs: Remarkable cooperation, persistence, and attention to detail. The hyperphagia requires environmental management, but the neurodiversity framework separates the person’s core identity from the medical complication.
Language note: Most self‑advocates with PWS prefer “person with Prader‑Willi syndrome” (person‑first). Always ask. Avoid “Prader‑Willi patient” or “suffers from.” The NNLM explicitly lists PWS as a neurotype, affirming that genetic syndromes are part of human neurodiversity, not separate from it.
Tourette Syndrome (TS)
Neurotype definition (Tourette syndrome as a neurotype):
A neurotype involving atypical development of cortico‑striato‑thalamo‑cortical (CSTC) circuits, particularly within the basal ganglia and dopaminergic system. This results in involuntary motor and vocal tics that are often preceded by a premonitory urge (sensory phenomenon). Critically, many people with TS also experience the “Tourette advantage”: heightened sensory awareness, rapid associative cognition, and a rich inner sensory‑linguistic world.
- Heritability: ~50–80% (polygenic, with possible auto‑immune subtypes).
- Key features: Tics that wax and wane (suppressible but not controllable), often with co‑occurring “non‑tics” such as echophenomena, coprophenomena (in a minority). High rates of creativity, humor, and out‑of‑the‑box thinking.
- Co‑occurrence: ADHD (50–70%), OCD (30–50%), autism, anxiety.
- Strengths/trade‑offs: Fast associative processing, heightened sensory scanning, resilience. Social mismatch arises from others’ reactions to tics, not from the tics themselves.
Language note: Many adults with TS prefer identity‑first (“Tourettic person” or “person with Tourette syndrome” – ask). Avoid “Tourette’s sufferer.” The NNLM includes TS as a neurotype, consistent with the view that movement differences are natural variations.
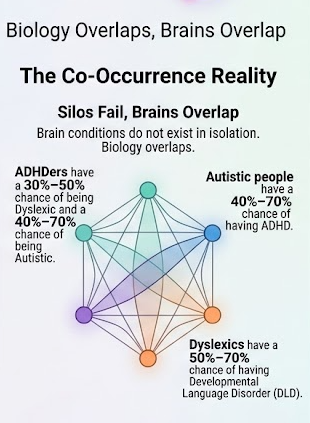
Co-occurrence Is the Rule, Not the Exception
Professor Amanda Kirby’s Neurodiversity Co-occurrence Map (Do-IT Solutions, 2024) visually demonstrates what clinical research has shown for decades: if you have one neurotype, the probability of having at least one other is high.
Why co-occurrence happens:
- Shared genetic variants (pleiotropy): Same genes affect multiple brain systems (e.g., FOXP2 affects language, motor, and attention).
- Overlapping brain circuits: Cerebellar-prefrontal loops are involved in motor coordination, attention, and timing—disruptions there contribute to DCD, ADHD, and dyslexia together.
- Cascading developmental effects: An early difference in sensory processing can alter social learning, which then affects attention or language.
Practical implication:
If you (or your child or employee) have one diagnosis, ask: What else is likely here? A person-centered, biopsychosocial approach beats siloed treatment every time (Kirby, 2024).
Language Matters: APA’s Inclusive Language Guide on Neurodiversity
The American Psychological Association’s Inclusive Language Guide (2nd ed., 2023) now includes an entire section on neurodiversity. This is a major shift from the purely deficit-based medical model.
Key points from the APA guide (2023, Neurodiversity section):
“Neurodiversity refers to the diversity of minds and brains that exist among all people… no two individuals have identical minds or brains, even people who would be categorized as ‘neurotypical’ are considered neurodiverse.”
“Neurodivergent… describes the idea that people experience and interact with the world around them in many ways; there is no one ‘right’ way of thinking, learning, and behaving, and differences are not viewed as deficits.”
The APA explicitly endorses:
- Identity-first language when preferred by the community (e.g., “autistic person,” “ADHDer”).
- Avoiding the term “neurodiverse” to mean “neurodivergent.”
- Recognizing that neurodivergence is not inherently pathological.
This aligns with the definitions from Nick Walker (2021) and the co-occurrence science from Kirby (2024).
Why This Matters Beyond Academia
When we use precise, neuroscience-informed language, we change practice:
- Education: Instead of “dyslexic student” in one room and “ADHD student” in another, we ask: What is this student’s full neurocognitive profile?
- Employment: Instead of accommodations for “autism” or “dyslexia” separately, we design for co-occurrence – flexible timing, quiet spaces, written and verbal instructions.
- Self-understanding: Instead of feeling “broken” for having multiple diagnoses, people see themselves as having a coherent, biologically expected neurotype cluster.
As the APA (2023) notes, “Neurodiversity-related discrimination is a specific type of ableism that can occur in the form of biases and expectations around cognitive functioning.” Changing our language is one step toward changing those expectations.
References
American Psychological Association. (2023). Inclusive language guide (2nd ed.). https://www.apa.org/about/apa/equity-diversity-inclusion/language-guidelines
American Speech-Language-Hearing Association. (n.d.). Developmental language disorder (DLD). https://www.asha.org/practice-portal/clinical-topics/developmental-language-disorder/
Asasumasu, K. (2000). Neurodivergent [Coined term]. In N. Walker (2021), Neurodiversity: Some basic terms & definitions. NeuroQueer.
Astle, D. E., Holmes, J., & Kievit, R. (2022). Annual Research Review: The transdiagnostic revolution in neurodevelopmental disorders. Journal of Child Psychology and Psychiatry, 63(4), 397–417. https://doi.org/10.1111/jcpp.13481
Bishop, D. V. M., Snowling, M. J., Thompson, P. A., & Greenhalgh, T. (2017). Phase 2 of CATALISE: A multinational and multidisciplinary Delphi consensus study of problems with language development. Journal of Child Psychology and Psychiatry, 58(10), 1068–1080. https://doi.org/10.1111/jcpp.12721 (Consensus definition of DLD)
Blank, R., Barnett, A. L., Cairney, J., Green, D., Kirby, A., Polatajko, H., Rosenblum, S., Smits-Engelsman, B., Sugden, D., Wilson, P., & Vinçon, S. (2019). International clinical practice recommendations on the definition, diagnosis, assessment, intervention, and psychosocial aspects of developmental coordination disorder. Developmental Medicine & Child Neurology, 61(3), 242–285. https://doi.org/10.1111/dmcn.14132
Butterworth, B., & Kovas, Y. (2013). Understanding neurocognitive developmental disorders can improve education for all. Science, 340(6133), 300–305. https://doi.org/10.1126/science.1231022 (Dyscalculia neural basis)
Do-IT Solutions. (2024). Neurodiversity co-occurrence map [Infographic]. Do-IT Profiler. https://doitprofiler.com/insight/neurodiversity-co-occurrence-map/
Doyle, N. (2020). Neurodiversity at work: A biopsychosocial model and the impact on working adults. British Medical Bulletin, 135(1), 108–125. https://doi.org/10.1093/bmb/ldaa021
Dwyer, P. (2022). The neurodiversity approach(es): What are they and what do they mean for researchers? Human Development, 66(2), 73–92. https://doi.org/10.1159/000523723
Faraone, S. V., Banaschewski, T., Coghill, D., et al. (2021). The World Federation of ADHD International Consensus Statement: 208 evidence-based conclusions about the disorder. Neuroscience & Biobehavioral Reviews, 128, 789–818. https://doi.org/10.1016/j.neubiorev.2021.01.022
Giraud, A. L., & Ramus, F. (2013). Neurogenetics and auditory processing in developmental dyslexia. Current Opinion in Neurobiology, 23(1), 37–42. https://doi.org/10.1016/j.conb.2012.09.003
International Dyslexia Association. (2025). Definition of dyslexia [Draft for 2025 revision]. https://dyslexiaida.org (Note: The 2025 draft was cited in our definition; the current official IDA definition remains 2002 but is under revision.)
Kirby, A. (2024). Neurodiversity co-occurrence: Why silos fail. Do-IT Insights. https://doitprofiler.com/insight/neurodiversity-co-occurrence-map/
Kucian, K., & Kaufmann, L. (2022). Developmental dyscalculia and the brain. In M. Danesi (Ed.), Handbook of cognitive mathematics (pp. 1–27). Springer. https://doi.org/10.1007/978-3-030-44982-7_10-1
National Library of Medicine. (2026). Neurodiversity [Reading club topic]. NNLM Reading Club. https://www.nnlm.gov/resources/reading-club/topic/331
National Institute of Mental Health. (2023). Attention-deficit/hyperactivity disorder (ADHD). https://www.nimh.nih.gov/health/topics/attention-deficit-hyperactivity-disorder-adhd
National Institute of Mental Health. (2024). Autism spectrum disorder. https://www.nimh.nih.gov/health/topics/autism-spectrum-disorders-asd
Petersen, I. T., & LeBeau, R. T. (2021). Co-occurrence of developmental disorders: A meta-analysis. Journal of Child Psychology and Psychiatry, 62(5), 514–529. https://doi.org/10.1111/jcpp.13319
Schneps, M. H., Brockmole, J. R., Sonnert, G., & Pomplun, M. (2012). History of reading struggles linked to enhanced learning in low spatial frequency scenes. Journal of Learning Disabilities, 45(5), 416–425. https://doi.org/10.1177/0022219411405501 (Dyslexia peripheral vision advantage)
Singer, J. (2017). NeuroDiversity: The birth of an idea. Kindle Direct Publishing.
Smith-Spark, J. H., & Fisk, J. E. (2022). Verbal and non-verbal memory in adults with developmental coordination disorder (DCD). Current Developmental Disorders Reports, 9(2), 31–38. https://doi.org/10.1007/s40474-022-00245-3
Walker, N. (2021). Neurodiversity: Some basic terms & definitions. NeuroQueer. https://neuroqueer.com/neurodiversity-terms-and-definitions/
Zwicker, J. G., Missiuna, C., & Boyd, L. A. (2019). Neural correlates of developmental coordination disorder: A review of the literature. Developmental Medicine & Child Neurology, 61(3), 247–253. https://doi.org/10.1111/dmcn.14056
Additional Recommended Resources (Not Cited Directly but Useful)
- American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). https://doi.org/10.1176/appi.books.9780890425787 (DSM‑5‑TR criteria for specific learning disorder, ADHD, autism, DCD, DLD – used clinically but reframed in this post)
- Kirby, A., & Smith, T. (2021). Neurodiversity at work: Drive innovation, performance, and productivity with a neurodiverse workforce. Kogan Page.
On giftedness as a neurotype:
Jung, R. E., & Haier, R. J. (2007). The Parieto‑Frontal Integration Theory (P‑FIT) of intelligence: Converging neuroimaging evidence. Behavioral and Brain Sciences, 30(2), 135–154. https://doi.org/10.1017/S0140525X07001185 (Neural efficiency and giftedness)
Lovecky, D. V. (2021). Different minds: Gifted children with ADHD, ASD, and other dual exceptionalities (2nd ed.). Jessica Kingsley Publishers. (Discusses giftedness as neurodivergence, though still uses “dual exceptionality” – useful transitional text.)
Ruf, D. L. (2023). The 5 levels of gifted children grown up: What they tell us. Gifted Unlimited. (Longitudinal study of gifted adults; supports heterogeneity.)
On multiply neurodivergent vs. 2e:
Kirby, A. (2024). Neurodiversity co‑occurrence map [Infographic]. Do‑IT Profiler. https://doitprofiler.com/insight/neurodiversity-co-occurrence-map/ (Shows that multiple co‑occurrence is the rule.)
Walker, N. (2021). Neurodiversity: Some basic terms & definitions. NeuroQueer. https://neuroqueer.com/neurodiversity-terms-and-definitions/ (Includes “multiply neurodivergent” as a term.)
On the shift away from 2e:
Baumer, N., & Frueh, J. (2021). What is neurodiversity? Harvard Health Blog. https://www.health.harvard.edu/blog/what-is-neurodiversity-202111232645 (Briefly discusses limitations of 2e framing.)
Comments ()